Sleep anxiety is the fear or worry about falling asleep or staying asleep. Over time, that fear can trigger a stress response at bedtime (hyperarousal), which makes sleep harder and reinforces the fear. Breaking the cycle involves lowering sleep’s “threat value,” rebuilding natural sleep drive, retraining the bed as a cue for sleep, and calming the nervous system using evidence-based behavioral sleep strategies.
TL;DR
Sleep anxiety is fear centered around sleep itself, not just “having insomnia.”
- It triggers hyperarousal at bedtime: racing thoughts, tension, heart pounding, clock-watching, and a sense that sleep is something you have to force.
- It can affect adults and children, often after a stretch of poor sleep, stress, schedule disruption, or a distressing night.
- It’s treatable. The most effective recovery approaches combine behavioral sleep retraining (including CBT-I principles), nervous system regulation, and circadian alignment.
- Breaking the anxiety–insomnia cycle means retraining your brain and body to experience bedtime as safe again, not trying harder to sleep.
- Supplements and medications may play a short-term role for some people, but they rarely address the conditioned fear that keeps sleep anxiety going.
Why Bedtime Can Feel Threatening
It often starts innocently. You have a few bad nights, a stressful week, or one “wide awake” evening that rattles you. Then bedtime changes.
The lights go out, and instead of feeling sleepy, you feel alert. Your heart rate jumps. Your mind starts negotiating: If I fall asleep right now, I can still get 6 hours. You check the clock. You calculate tomorrow’s damage. You try to force sleep, and your body responds as if you are facing a threat.
That experience is real, common, and highly treatable.
At Sleep Science Academy, we teach evidence-based sleep education and behavioral sleep medicine principles used in clinical settings. CBT-I provides an important foundation, but we also emphasize circadian science, nervous system regulation, conditioning, and habit retraining as part of a comprehensive approach.
What Is Sleep Anxiety?
Sleep anxiety is a conditioned fear response around bedtime, sleep, or the act of trying to sleep. Some people call it somniphobia, but many cases are not a true phobia. More commonly, it is learned “sleep performance anxiety.”
Insomnia vs Sleep Anxiety
- Insomnia describes symptoms: trouble falling asleep, staying asleep, or waking early with daytime impairment.
- Sleep anxiety is often a major driver and maintainer of insomnia: fear of another bad night, fear of next-day consequences, fear of lying awake.
In other words, insomnia can begin for many reasons (stress, schedule changes, illness), but it often becomes chronic because the brain starts treating bedtime like a threat.
Overlap Without Over-Pathologizing
Sleep anxiety can overlap with:
- Generalized Anxiety Disorder (GAD)
- Panic disorder (including nocturnal panic)
- Depression (sleep disruption and mood changes reinforce each other)
- Health anxiety (hyper-monitoring bodily sensations at night)
You can have sleep anxiety without having an anxiety disorder. And you can have an anxiety disorder without having sleep anxiety. The pattern matters.
You Might Have Sleep Anxiety If…
- You feel dread when you think about going to bed
- You start “calculating sleep” and monitoring the clock
- You feel physically wired once you get into bed
- You avoid bed, delay bedtime, or “revenge scroll” because you fear the moment you try to sleep
- You feel safer on the couch, in a different room, or with the TV on
- You rely on a safety behavior (pill, alcohol, special routine, wearable stats) to feel like sleep is possible
Why Bedtime Becomes a Trigger
Your brain learns through association. After enough nights of struggle, the bed stops being a cue for sleep and becomes a cue for alertness. That is not a willpower problem. It is basic learning and physiology.
Sleep Anxiety Symptoms
Sleep anxiety can look mental, physical, and behavioral. Many people experience all three.
Common mental symptoms
- Racing thoughts, repetitive worries, rumination
- Dread about being awake
- Catastrophic predictions about tomorrow
- Hyper-focus on whether you feel sleepy “enough”
- Intrusive thoughts like “What if I never sleep again?”
Physical Symptoms (Sympathetic Activation)
- Racing heart or pounding pulse
- Muscle tension (jaw, shoulders, stomach)
- Sweating or hot flashes
- Stomach discomfort, nausea, “butterflies”
- Restlessness, twitching
- Chest tightness or a sense of air hunger
- Tingling, buzzing, or “adrenaline” sensations
- Jolting awake right as you drift off (a common hyperarousal sign)
These sensations are often interpreted as danger, which adds more fear. But in many cases they are simply the body’s stress system doing its job at the wrong time.
Behavioral Symptoms
- Clock-watching (including “just one quick check”)
- Avoiding bed or delaying bedtime
- Excessive sleep tracking (wearables, apps, constant scoring)
- Over-researching sleep late at night
- Taking sedatives or alcohol “just in case”
- Spending excessive time in bed to “catch up”
Quick checklist summary: If bedtime reliably triggers worry + body arousal + monitoring behaviors, sleep anxiety is likely part of the picture.
Why Sleep Anxiety Gets Worse at Night: The Science in 3 Layers
Sleep anxiety intensifies at night for predictable reasons. Here is the simplest evidence-based way to understand it.
Layer 1: Biology (timing, arousal systems, and attention)
- Your circadian rhythm changes what your brain and body expect across the day and night.
- Stress can shift arousal patterns. When you are under pressure, the body’s alerting systems can stay more active at night.
- Lying still in the dark amplifies internal sensations (heartbeats, breathing changes, muscle tension). If you are scanning for signs of sleep, you will notice everything.
Layer 2: Learning (conditioning and “trying” backfires)
When the bed becomes associated with struggle, the brain learns: bed = problem-solving zone.
That is classical conditioning in action. And then a second trap appears: the harder you try to force sleep, the more alert you become. This is why approaches like paradoxical intention (reducing the effort to sleep) can help some people. Sleep is not a performance. It is a biological process that shows up when conditions are right.
Layer 3: Behaviors (safety behaviors keep fear alive)
Safety behaviors reduce anxiety in the short term, but they prevent learning in the long term. Common examples:
- Going to bed early “to increase chances”
- Checking the clock to feel in control
- Scrolling to distract yourself
- Sleeping pills as a security blanket
- Canceling plans the next day “because you won’t sleep”
These behaviors teach your brain that sleep is dangerous and you need protection.
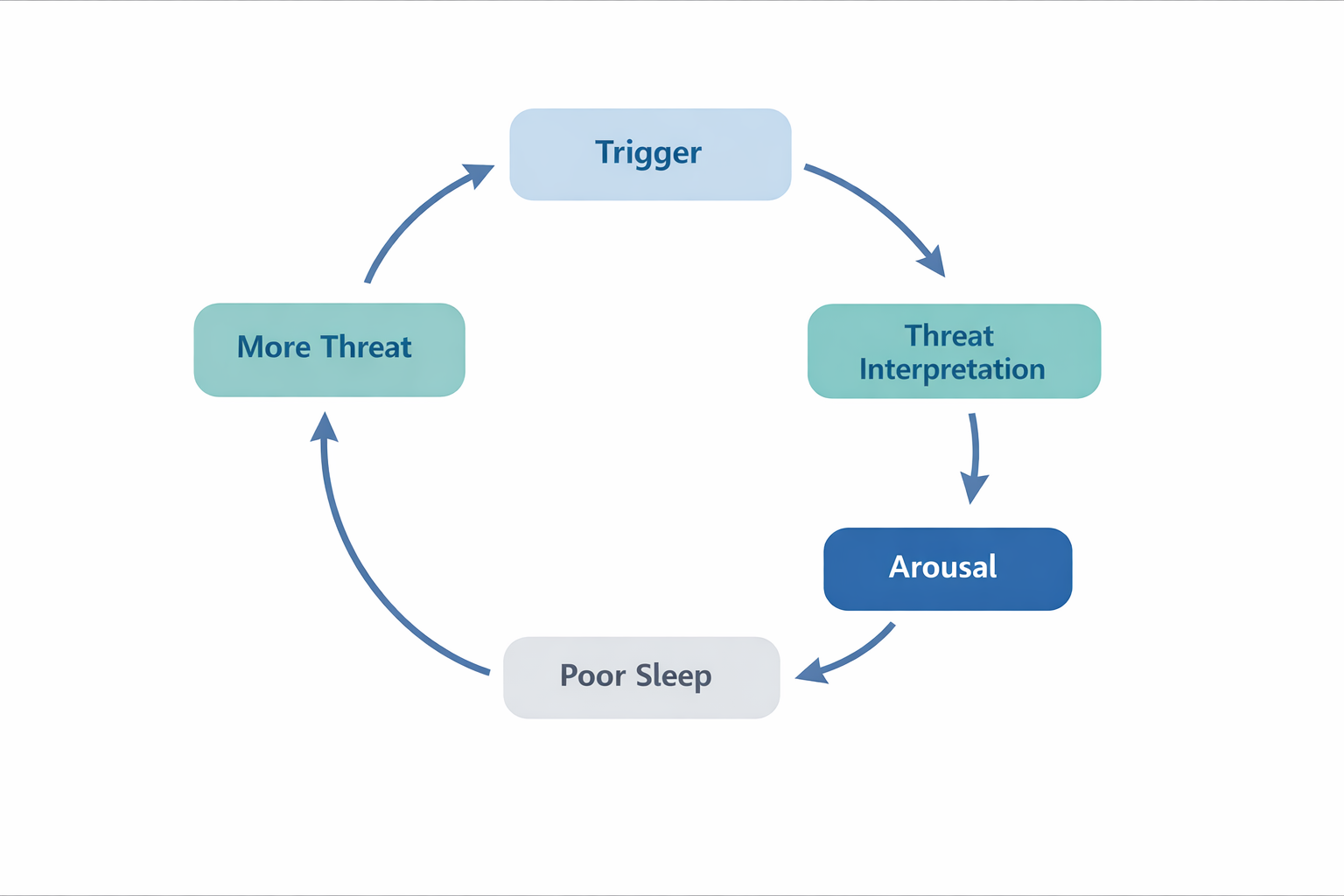
Hyperarousal cycle that maintains insomnia
Effective recovery usually means addressing all three layers together, biology, learning, and behavior, rather than focusing on just one.
Common Causes and Contributors: The ‘Sleep Anxiety Checklist’
Sleep anxiety is often multi-factorial. Use this checklist to identify contributors you can modify.
Stimulants and Timing
- Caffeine: Amount, timing, and sensitivity all matter. Even morning caffeine can affect some sensitive sleepers.
- Nicotine: Stimulating and associated with lighter sleep.
- Pre-workout supplements: Often contain high-dose caffeine and other stimulants.
- ADHD medications: Timing can matter; discuss adjustments with a prescriber if sleep is affected.
Sleep Environment and Schedule Instability
- Temperature (many people sleep best in a cool room)
- Noise and light exposure
- Partner snoring
- Travel, jet lag
- Shift work or irregular schedules
- Inconsistent wake times (even if bedtime varies)
Life Events and Mental Health Factors
- Grief, caregiving stress, burnout
- Postpartum changes
- Depression and anxiety (bidirectional relationship with sleep disruption is well established in sleep research)
If your sleep anxiety started “out of nowhere,” it is still worth checking for a new stressor, a schedule shift, or a hidden medical contributor.
Sleep Apnea and Anxiety: The Overlap People Miss
Untreated obstructive sleep apnea (OSA) can mimic or worsen anxiety because it repeatedly triggers micro-arousals and stress responses during sleep.
People with OSA may experience:
- Repeated awakenings they do not remember
- Adrenaline surges at night
- Morning headaches
- Daytime fatigue that feels like anxiety
- Panic-like symptoms upon waking
Red Flags That Suggest Apnea
- Loud, chronic snoring
- Witnessed pauses in breathing
- Gasping or choking during sleep
- High daytime sleepiness
- High blood pressure
- Waking with dry mouth or headaches
Anxiety can also worsen the sensation of breathing discomfort at night, so it is easy to mislabel everything as “just anxiety.” If these red flags fit, talk to a clinician. In many regions, home sleep apnea testing is an accessible first step when appropriate.
Sleep Anxiety in Children
Sleep anxiety in children often appears as resistance at bedtime, fear of being alone, and repeated requests for reassurance. These behaviors can be mistaken for other problems, making it harder to address the true cause. Common signs include stalling at bedtime, needing a parent nearby to sleep, waking and calling out during the night, and fears like darkness or nightmares.
The recommended approach is to combine warmth with consistent routines; offering support without creating endless reassurance cycles. Parents are encouraged to keep bedtime routines short and predictable, practice coping skills during the day, gradually space out check-ins, avoid relying on screens for comfort, and praise brave efforts rather than focusing on sleep itself.
If a child experiences loud snoring, gasping, restless sleep, persistent insomnia, or significant daytime issues, involving a pediatrician or therapist is advised.
The Sleep Anxiety Cycle and How to Break It
Sleep anxiety doesn’t just appear out of nowhere. It builds its own momentum through a self-reinforcing loop. When fear of sleeplessness creeps in, it changes how your mind and body react at night, making restful sleep even harder to achieve. Here is the cycle in plain language:
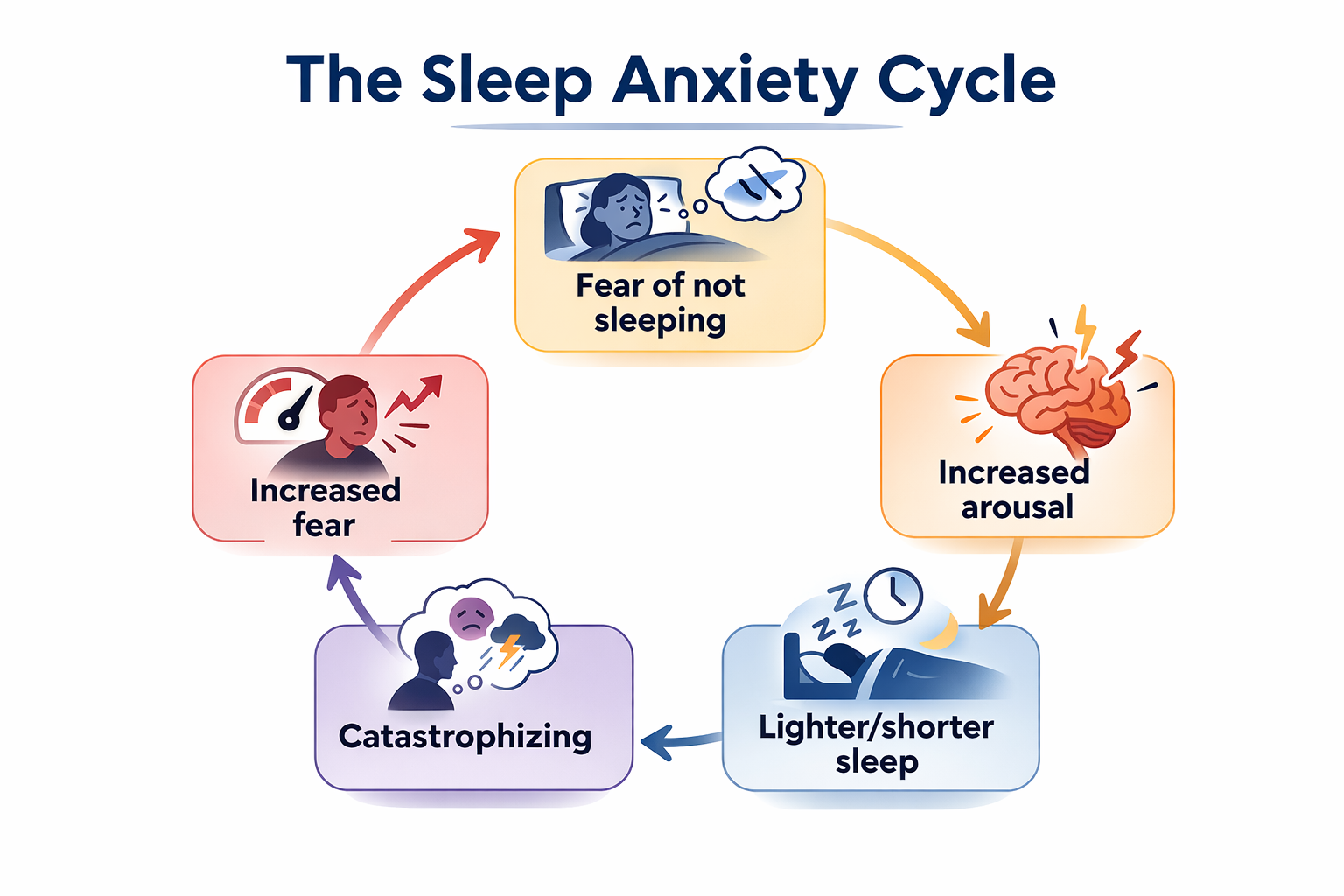
A visual overview of how nighttime worry can quietly reinforce and perpetuate insomnia.
The way out is not accumulating more sleep hacks. It is gradually retraining your brain and nervous system to experience bedtime as safe again.
A CBT-I Aligned Framework (Step-by-Step)
CBT-I is considered a first-line behavioral treatment for chronic insomnia by major medical guidelines and is supported by decades of research. Its core principles: stimulus control, sleep efficiency, cognitive restructuring, and consistent timing, form the backbone of most effective sleep anxiety interventions.
You do not need to do every step perfectly. You do need to do a few core steps consistently.
- Reduce time-in-bed mismatch: If you spend 9–10 hours in bed trying to get 7 hours of sleep, you often train lighter, more fragmented sleep and more time for worrying. Improving sleep efficiency is often part of recovery.
- Rebuild sleep drive: Sleep pressure builds the longer you are awake. Consistent wake time and appropriate time-in-bed help sleep pressure do its job.
- Retrain “bed = sleep” (stimulus control): The bed should become boring again: a cue for sleep and intimacy, not worry, work, scrolling, or clock-checking.
- Change worry habits: Sleep anxiety is often a worry habit that shows up at night. You will interrupt it with scheduled worry, reframing, and “permission to be awake” practice.
- Lower physiologic arousal: Breathing, PMR, and grounding reduce the body’s threat response so sleep can arrive.
Do This Tonight: A 15–30 Minute Anti-Anxiety Wind-Down Protocol
This is a practical routine designed to be repeated each night. Consistency is more important than doing every step perfectly. Regular practice is what brings lasting results.
60 Minutes Before Bed (Set the Stage)
- Dim lights and lower stimulation
- Keep screens calmer and warmer if you use them (avoid doom scrolling or intense content)
- Avoid caffeine late in the day; avoid alcohol close to bedtime if it worsens awakenings
- No clock-checking once you start your wind-down (turn the clock away)
30 Minutes Before Bed (Clear the Mental Load)
Brain dump (5–10 minutes):
- “What’s on my mind”
- “Next action I can take” (one small step per item)
- “What can wait until tomorrow”
Then choose a low-key activity: reading something light, stretching gently, a warm shower, or prepping for tomorrow.
10 Minutes Before Bed (Downshift the Body)
Pick one:
- Resonance breathing (5–6 breaths/min): Slow, steady breaths at this pace help calm the nervous system and ease physical arousal before bed.
- Progressive muscle relaxation: Briefly tense and relax muscle groups to release physical tension and promote a sense of relaxation.
- Body scan meditation: Gently focus attention on different parts of your body, grounding you in the present and reducing anxious thoughts.
Breathing Exercises for Sleep Anxiety
Slow breathing can reduce sympathetic activation and increase parasympathetic influence (vagal tone). It is a reliable way to nudge the nervous system toward safety.
If you feel dizzy, breathe more gently and slow down. If you have respiratory or cardiac conditions, ask your clinician what is appropriate.
1) Resonance Breathing (5–6 Breaths Per Minute)
Best for: general bedtime arousal, restless body
How to do it (5–10 minutes):
- Sit or lie comfortably.
- Inhale through the nose for 4–5 seconds.
- Exhale slowly for 5–6 seconds.
- Keep shoulders soft; breathe low into the belly and ribs.
- If your mind wanders, return to counting.
2) Physiological Sigh (Fast Reset for Spikes)
Best for: sudden panic surge, heart racing
How to do it (1–2 minutes):
- Inhale through the nose.
- At the top, take a second inhalation to “top up.”
- Exhale long and slow through the mouth.
- Repeat 2–5 times, then switch to slow breathing.
3) Extended Exhale Breathing
Best for: falling asleep, reducing threat scanning
How to do it (3–5 minutes):
- Inhale 4 seconds, exhale 6–8 seconds.
- Make the exhale smooth, not forced.
Progressive Muscle Relaxation (PMR) + Body-Based Techniques
PMR helps by lowering somatic tension and teaching your body the difference between “on” and “off.”
Full PMR (10 Minutes)
Move from feet to face:
- Tense feet for 5 seconds, release for 10 seconds.
- Calves, thighs, glutes.
- Belly, hands, arms, shoulders.
- Jaw, eyes, forehead.
You are aiming for gentle tension, not cramping.
Short PMR for Middle-of-the-Night Awakenings (2 Minutes)
- Shrug shoulders up for 3 seconds, release.
- Clench fists for 3 seconds, release.
- Press toes down for 3 seconds, release.
- Slow exhale after each release.
Other Body-Based Options (Low Stimulation)
- Gentle stretching or mobility (avoid vigorous exercise close to bed)
- Warm shower or bath earlier in the evening
- Weighted blanket considerations: may help some people feel grounded; avoid if it worsens breathing, overheating, or mobility issues
Grounding techniques for acute anxiety
- 5-4-3-2-1 senses: name 5 things you see, 4 feel, 3 hear, 2 smell, 1 taste
- Press feet into the floor and notice pressure points
- Temperature shift: cool cloth on the face or back of the neck
Meditation for Anxiety and Sleep
Meditation is not about forcing sleep; it is about changing your relationship to wakefulness. For sleep anxiety, the win is learning to stop monitoring for sleep and stop treating wakefulness as danger.
Best-Fit Approaches for Sleep Anxiety
- Mindfulness of breath (simple anchor)
- Body scan (reduces scanning for threat)
- Loving-kindness (helpful for self-criticism and “I’m failing at sleep” narratives)
- Acceptance-based approaches (ACT-style): making room for wakefulness without struggle
What Tends to Backfire
- Using meditation as a performance tool: “If I do this perfectly, I’ll fall asleep”
- Long, intense sessions in bed that increase effort and frustration
- Forcing silence when you do better with gentle sound
Simple 7-Minute Script Outline
- Settle: “Let the bed hold your weight.”
- Anchor: feel the breath at the nose or belly.
- Label thoughts: “planning,” “worrying,” “judging.”
- Return: back to breath, no debate.
- Expand: scan the body, soften jaw and shoulders.
- Close: “Tonight my job is to rest. Sleep can come on its own.”
For guided options, look for reputable health systems, university programs, or well-reviewed meditation apps. Prioritize content that is calm, evidence-informed, and not packed with dramatic promises.
Adjunct Tools (Not Core Treatment)
Best Vitamins for Sleep and Anxiety

Supplements for sleep and anxiety support
Supplements can support overall health when deficiencies are present, but they rarely resolve conditioned sleep anxiety on their own.
Commonly discussed nutrients:
- Vitamin D: plausible if deficient; deficiency is common in some populations and may correlate with mood and sleep issues.
- B12 and folate: deficiencies can affect energy, mood, and neurologic function.
- Iron: important if restless legs symptoms are present; check ferritin with a clinician.
- Magnesium: a mineral often discussed for relaxation; evidence is mixed, and dosing should be cautious.
- Omega-3s: some evidence for mood support; not a direct sleep anxiety treatment.
Practical approach
- If sleep anxiety is persistent, consider basic labs with a clinician if indicated.
- Avoid stacking multiple products at once. You will not know what helped, and you may increase side effects.
Binaural Beats
Binaural beats are an audio illusion created when each ear hears a slightly different tone, and the brain perceives a third “beat.” Some people find them relaxing. Research is mixed, and effects are generally small and individual.
Practical guidance if you try them
- Use low volume
- Use stereo headphones (required for the effect)
- Stop if you get headaches or increased anxiety
- Treat this as optional. If you have chronic insomnia, prioritize CBT-I skills first.
Cognitive Tools: Stop the Worry Loop Before It Hits the Pillow
If sleep anxiety stems in part from a habit of worrying, it’s crucial to establish a structured worry routine that takes place well before bedtime. This proactive approach helps prevent anxious thoughts from dominating your mind when you’re trying to fall asleep.
1) Scheduled Worry (15 Minutes, Earlier in the Evening)
Set a timer. Then split concerns into two columns:
Problems I can act on
- Write the next step (one small action)
Problems I can’t solve tonight
- Write an acceptance line: “This is here. I will handle it tomorrow.”
This trains your brain that nighttime is not the time for problem-solving.
2) Brain Dump Protocol
On paper:
- What’s on my mind
- Next action (if any)
- Park it for tomorrow
The goal is not perfect organization. It is containment.
3) Cognitive Restructuring (Catastrophe to Balance)
Common thought: “If I don’t sleep, I’ll fail tomorrow.”
Balanced replacement: “I might feel tired, but I’ve functioned on less sleep before. I can do the essentials, and tomorrow night I can still sleep.”
The goal is to bring the fear back into proportion and respond with a balanced, realistic perspective.
When Sleep Anxiety Signals Something Bigger
Consider professional support if you notice:
- Insomnia persisting more than 3 months
- Significant daytime impairment (work, driving, mood, functioning)
- Symptoms of depression, especially hopelessness or suicidal thoughts
- Trauma symptoms or severe panic
- Reliance on alcohol, cannabis, or sedatives to sleep
- Suspected sleep apnea (snoring, gasping, witnessed pauses)
For Sleep Coaches and Health Professionals
Sleep anxiety is one of the most common maintaining factors in chronic insomnia. Understanding conditioned arousal, circadian biology, nervous system regulation, and behavioral retraining is essential when working with clients struggling with persistent sleep fear.
At Sleep Science Academy, we teach these principles as part of a comprehensive behavioral sleep science framework designed for practitioners and coaches seeking deeper training.
Building a Calmer Relationship with Sleep
Sleep anxiety is a learned fear response around bedtime. You treat it by reducing the threat value of nighttime, rebuilding sleep drive through consistent timing, retraining the bed as a cue for sleep, and interrupting worry and safety behaviors. Tools like breathing, PMR, and mindfulness help regulate arousal, but lasting change typically comes from addressing conditioned fear, circadian timing, and behavioral patterns together.
FAQs
Can anxiety cause sleep loss?
Yes. Anxiety can trigger hyperarousal, making it harder to fall asleep or stay asleep. Worry, threat scanning, and physical tension can reduce sleep depth and increase awakenings. Addressing both the anxiety process and sleep behaviors (often with CBT-I) is typically most effective.
Can lack of sleep cause anxiety?
Yes. Poor sleep can increase emotional reactivity and stress sensitivity the next day. This can make worries feel louder and coping feel harder. That bidirectional loop is why breaking the sleep anxiety cycle often reduces daytime anxiety as well.
Can sleep apnea cause anxiety or panic attacks at night?
It can. Obstructive sleep apnea causes repeated breathing disruptions and arousals that may feel like nighttime panic, gasping, or adrenaline surges. Loud snoring, witnessed pauses, and choking awakenings are key red flags. If suspected, talk with a clinician about evaluation options.
What triggers sleep anxiety?
Common triggers include a period of insomnia, stress, grief, burnout, irregular schedules, stimulant use, alcohol-related sleep fragmentation, and conditioning from repeated nights of struggle. Safety behaviors like clock-checking and going to bed early can also maintain sleep anxiety over time.
Does melatonin help anxiety-related insomnia?
Melatonin primarily helps with circadian timing (when your body feels sleepy) rather than directly treating anxiety. Some people find it useful, especially for delayed sleep schedules or jet lag, but it is not a primary treatment for sleep anxiety. For chronic insomnia, CBT-I strategies are usually more effective long-term.
What color noise is best for sleep and anxiety?
There is no single “best” color noise for sleep and anxiety, but pink noise is commonly associated with improved sleep stability. Pink noise reduces higher-frequency sound intensity, which may decrease micro-arousals and support more consistent slow-wave sleep. For individuals with anxiety-related hyperarousal, steady broadband sound can mask environmental disruptions and reduce conditioned arousal at bedtime. Preference and individual nervous system sensitivity often determine which sound is most calming.
What is the 3-3-3 rule for anxiety sleep?
The 3-3-3 rule is a grounding technique used to reduce acute anxiety before sleep. It typically involves identifying three things you see, three things you hear, and moving three parts of your body to shift attention away from worry. This sensory redirection may reduce amygdala activation and interrupt cognitive hyperarousal that delays sleep onset. While not a sleep treatment, it can complement cognitive behavioral therapy for insomnia (CBT-I) strategies.
What medication is used for sleep anxiety?
Several medication classes are used for sleep-related anxiety, including short-term hypnotics, certain antidepressants, and occasionally anti-anxiety agents. These medications often target neurotransmitter systems involved in arousal regulation, such as GABA or serotonin pathways. They may reduce nighttime hyperarousal but do not address conditioned arousal or circadian timing factors that commonly maintain insomnia. Behavioral approaches like CBT-I are often recommended alongside or instead of medication in long-term management.
Why does anxiety get worse at night?
Anxiety often feels worse at night because external distractions decrease and internal threat monitoring increases. In a dark, quiet environment, cognitive rumination and amygdala-driven threat processing can intensify, especially when the body is already in a state of hyperarousal. Disruption of normal cortisol rhythm and irregular circadian timing may further amplify nighttime alertness. Repeated nights of difficulty can also create conditioned arousal, reinforcing the brain’s association between bed and stress.